Common questions
Frontal lobe – is at the front of the brain (yellow section below).
It is responsible for:
- Problem solving
- Planning and organising
- Making judgements
- Emotions, behaviour and mood
- Personality
- Social skills
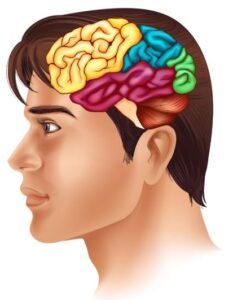
Parietal lobe – is on the top, back of the brain (blue section below).
It is responsible for:
- Knowing left from right
- Sensations (touch, pressure, temperature, pain)
- Hearing
- Reading
- Smelling
- Tasting
- Touch
- Understanding what we see
- Reading and writing
- Understanding shapes, colour and distance
- Understanding language
- Memory
- Emotions
- Enjoyment of music
- Recognising and identifying things we see (faces or objects)
- Balance
- Coordination
- Movement
- Regulating feelings and responses
- Organising thought
- Breathing
- Swallowing
- Appetite
- Beating of our heart
- Body temperature
- Staying awake or asleep
How do the different parts of our brain work together?
All lobes work together for you to do the things you do every day.
Here’s an example of getting ready for school:
| Frontal | Temporal | Parietal | Occipital | |
| Remembering what time school starts |  |
|
|
|
| Using watch to check the time | |
|
|
|
| Remembering where your classroom is and how to get there |  |
|
|
|
| Walking to your desk and sitting down | |
|
|
|
| Recognising your friends and teacher | |
|
|
|
| Listen for your name and responding | |
|
|
|
Stroke
A stroke is when there is not enough blood in the brain. It could be because:
 |
The heart may not be able to pump blood to the brain very well so the blood forms sticky clumps that causes a blockage. Doctor’s call these clumps ‘clots’
|
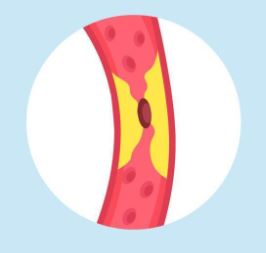 |
Sticky clumps or fat may build up inside the tubes and stop the blood from flowing |
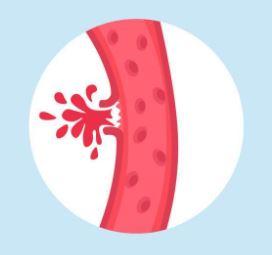 |
One of the tubes going to the brain tears a little bit and some blood leaks out |
Other ways a stroke can happen are:
- Some of the tubes going to the brain are a bit tangled up so blood gets stuck
- Some of the tubes going to the brain are a bit small and thin so blood gets stuck
Car accident

In a car accident, people’s head usually gets hit or moves very fast and suddenly stops. When this happens, the brain inside the skull can get hurt. Even though the brain is protected by the skull, it’s soft and can bump against the inside of the skull during a crash. This can cause bruising, swelling, or tiny tears in the brain.
Brain tumour
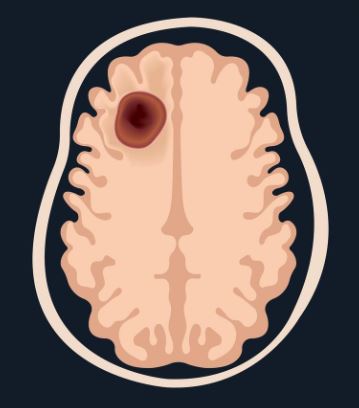
A brain tumour is a lump of cells that grows in the brain and shouldn’t be there. It happens when some cells start to grow too much or in the wrong way. Some brain tumors grow very slowly and might not cause many problems, while others can grow faster and press on parts of the brain, making it harder to think, move, or feel normal. Doctors use special tests and treatments to help people with brain tumors feel better and keep the brain working well.
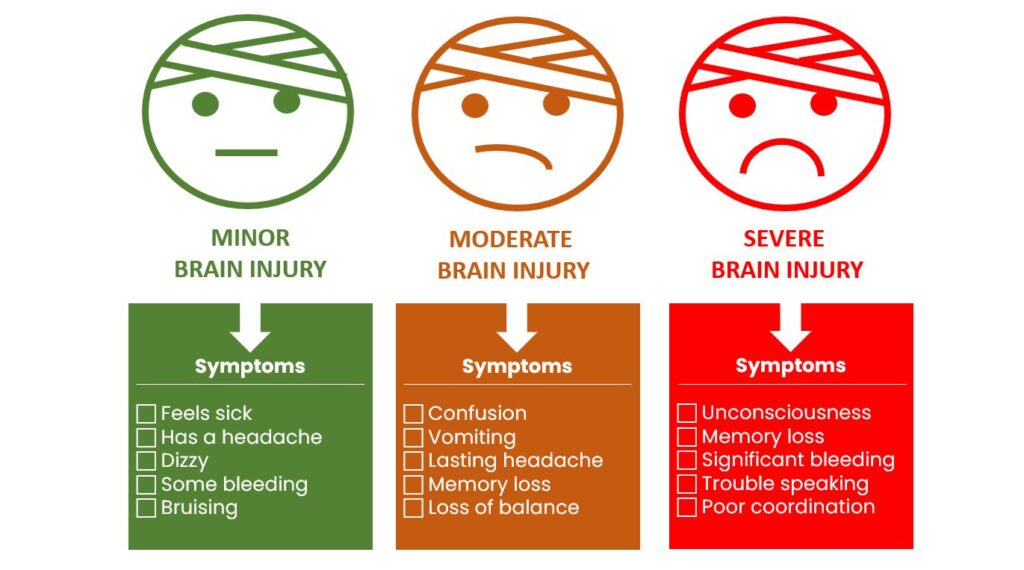
Different tests done in the hospital will help to know how big the brain injury may be.
The more serious the injury, the longer your special person will likely stay in hospital.
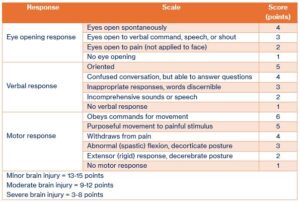
When someone experiences a brain injury, paramedics and doctors often check something called the Glasgow Coma Scale (GCS). It’s a simple way of seeing how awake, aware and responsive a person is right after the injury. The test looks at 3 things: how well the person opens their eyes, how they speak, and how they move.
The score helps them understand how serious the injury might be and what kind of care is needed.
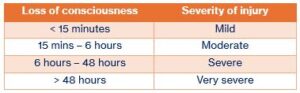
When someone has a brain injury, they might lose consciousness for a short time, a long time, or not at all. This simply means how long they were “out” or unaware of what was happening.
The length of time someone is unconscious is one of the clues doctors use to understand how serious the injury may be. Some people wake up quickly, some take longer, and every person’s recovery is different.
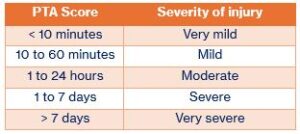
When someone experiences a traumatic brain injury (TBI), they might go through a phase of recovery called Post-Traumatic Amnesia (PTA). This is a period when they will feel confused, forget things that just happened, or not remember where they are of what day it is. PTA can last minutes, hours, or weeks which is normal for the stage of recovery.
The length of PTA helps doctors understand how serious the injury may be and what kind of support the person might need.
Rehabilitation specialists, registrars and medical officers are responsible for the medical care of your special person. The doctor’s main roles in rehabilitation are:
- Liaising with consultants in other medical specialists
- Medical management
- Reviewing progress
- Educating patients and families

Nurses provide around the clock care, support and expertise to your special person. Their main roles in rehabilitation are:
- Emotional support
- Monitoring vital signs to prevent complications
- General nursing care
- Assistance with transfers and mobility
- Personal care such as showering and grooming
- Toileting
- Eating and nutrition

An Occupational Therapist (OT) helps to regain, develop or maintain the skills needed for daily living and working, focusing on enabling your special person to perform everyday activities. Their main roles in rehabilitation are:
- Driving assessment and retraining
- Assessing independence in every day tasks
- Teaching techniques to maximise independence
- Using activities to treat physical and thinking challenges
- Home assessments
- Discharge Planning
- Splinting
- Scripting of aids or wheelchairs
- Return to work or study

A PT specialises in improving movement, function and overall physical wellbeing through targeted exercises, manual therapy and education. Their main roles in rehabilitation are:
- Hydrotherapy
- Individual and group therapies
- Assessment of indoor and outdoor mobility
- Assess balance problems
- Physical conditioning
- Discharge Planning

Social Workers (SW) assist individuals, families and children in navigating and overcoming social, emotional and economic challenges by providing support, resources, and advocacy to improve overall well-being and quality of life.
Their main roles are:
- Emotional support and counselling
- Practical assistance
- Connection to services and funding bodies
- Discharge planning

A Speech Pathologist (SP) assesses and treats communication and swallowing disorders, helping your special person to improve their speech, language and cognitive-communication skills. Their main roles in rehabilitation are:
- Assessing and treating communication problems
- Management of swallowing problems
- Discharge Planning

Aphasia happens when the part of the brain that controls language gets hurt.
A person with aphasia may have a hard time understanding, speaking, reading or writing.
Aphasia does not change intelligence.
There are 2 types of aphasia:
- Expressive – having a hard time producing words or saying what they’re thinking
- Receptive – having a hard time understanding what they hear or read
Imagine you know exactly what you want to say, but the words just don’t come out right or they come out in a funny order. It’s like being asked a question and having all your words stuck, like in a game of scrabble…all mixed up and out of reach. That would be frustrating right?! That’s what people with aphasia often go through every day.
Aphasia can change someone’s independence, and learning which can be frustrating. Some things may be hard to do, such as:
- Talking with family and friends
- Telling people about their thoughts and feelings
- Understanding what is said and following instructions
- Remembering what was said
- Finding the right words
- Concentrating when someone is talking
- Being able to write or talk
- Understanding jokes
- Feel alone, frustrated or not as confident

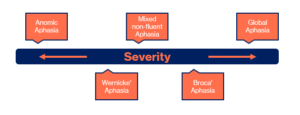
There are a few different types of aphasia, each with their own unique challenges. Here are a few of them:
- Non-fluent Aphasia People with this type know what they want to say but can’t get the words out smoothly. They might speak in short phrases, kind of like texting shorthand — ‘Want water’ instead of ‘I would like a glass of water.’ Reading and writing could be a bit hard too. They can still understand others, though!
- Fluent Aphasia This type is a little different. People with Wernicke’s aphasia can talk easily, but sometimes the words don’t make much sense. It’s like saying ‘couch on the moon’ when they mean ‘let’s go sit outside.’ Understanding others can be tough for them, too and reading and writing might be tricky.
- Global Aphasia This one is more severe. People with global aphasia have lots of trouble with speaking, understanding language and reading and writing. But with support, they can still connect with others through gestures, expressions, and patience.

Still can’t find what you’re looking for?
Lorem ipsum dolor sit amet, consetetur sadipscing elitr, sed diam nonumy eirmod tempor invidunt ut labore et dolore magna aliquyam erat, sed diam voluptua. At vero eos et accusam et justo.
Contact us